No need for surgery
Cook et al. investigated a new form of neuromodulation therapy for individuals with psychiatric disorders. Significant improvements in depression and posttraumatic stress disorder symptoms were observed after acute external trigeminal nerve stimulation treatment.
Author: Tamsen Hutchison
Download: [ PDF ]
Neurophysiology
In a paper published on January 28, 2016 in Neuromodulation, Cook et al. investigated the effectiveness of an 8-week external trigeminal nerve stimulation intervention on posttraumatic stress disorder (PTSD) and major depressive disorder (MDD) symptoms.1 Recent estimates for the prevalence of PTSD in the U.S. suggest that approximately 3.5% of the population is affected by the disorder.2 The symptoms associated with PTSD can have a detrimental effect on quality of life, putting individuals at a higher risk of suicide.3 Common treatments for PTSD symptoms are medications, such as selective serotonin reuptake inhibitors (SSRIs), or psychosocial interventions, such as cognitive behavioral therapy.4 However, even when these treatments are combined, the majority of patients do not experience significant improvement in their symptoms.5 The motivation behind this research was influenced by the lack of effective treatments for patients with co-occurring PTSD and MDD. The researchers found that severity of depression and PTSD symptoms improved over the course of the 8-week external trigeminal nerve stimulation (eTNS) treatment. These results imply that neuromodulation therapy may be an effective new approach for the treatment of psychiatric disorders.6
External trigeminal nerve stimulation therapy can be used to send signals to the brain by stimulating the trigeminal nerve with small electrical currents.7 One of the regions from which the trigeminal nerve transports signals is from the face to the nucleus tractus solitarius (NTS). The NTS is located in the brainstem and is believed to be responsible for integrating and relaying signals to structures that are associated with PTSD.8 In previous studies, symptoms of fear and depression have been significantly improved by treatment with eTNS.9,10
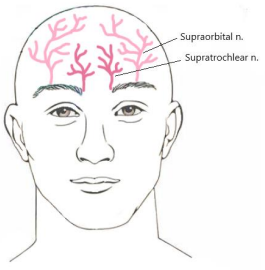
For this experiment, the researchers recruited 12 individuals (8 women and 4 men) between the ages of 18 and 75 who displayed symptoms of PTSD and MDD. In order to meet this criterion, the participants had to score a minimum of 14 of the 17-item Hamilton Depression Rating Scale (HDRS-17) and at least 50 on the Clinical-Administrated PTSD Scale (CAPS). Prior to the TNS intervention, participants were assessed for baseline PTSD and depression severity using the PTSD Patient Checklist (PCL), HDRS-17, and the Quick Inventory of Depressive Symptomatology (QIDS-C). These measures were then reassessed after 2 weeks, 4 weeks, 6 weeks, and 8 weeks of eTNS therapy. Scores from the Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q) were used to assess quality of life at baseline and again at week 8. During the TNS intervention, the participants were instructed to place electrodes on their forehead and to stimulate the supraorbital and supratrochlear nerves (depicted in Figure 1) each night for eight hours. The stimulation used for this experiment had a frequency of 120 Hz, a pulse width of 250 µsec, and was cycled on and off for 30 seconds at a time.
The results of the 8-week TNS intervention showed significant decreases in the negative symptoms associated with PTSD and MDD. Scores for the PCL averaged at 43.0 at week 8 compared to the 63.3 at baseline, indicating an improvement in PTSD characteristics. Improvement in depression severity was also observed following the 8- week TNS intervention. HDRS-17 scores dropped from a baseline average of 25.3 to 11.9 at week 8, and QIDS-C scores dropped from 17.8 to an 8.8 by the end of the intervention. Scores for quality of life also revealed significant improvement, with an average final score of 50.1 compared to 38.4 at baseline.
The results display evidence to support eTNS therapy for the treatment of individuals with comorbid PTSD and MDD. Neuromodulation treatments using external devices are beneficial because they are convenient, easy to use, and they do not require the patient to undergo any invasive surgical implantations.11 This study also found that this method of treatment resulted in mild or no side effects, and that all participants considered the treatment to be safe and acceptable for clinical use. Future research in the field should focus on the mechanisms that are involved in the treatment of psychiatric disorders through neuromodulation. In addition, future research would benefit from obtaining a larger sample size and from including a control group to avoid a potential placebo effect from occurring.
[+] References
Cook, I. A., Abrams, M., & Leuchter, A. F. (2016). Trigeminal nerve stimulation for comorbid posttraumatic stress disorder and major depressive disorder. Neuromodulation: Technology at the Neural Interface, 19: 299-305
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry, 62: 593-602
Kessler, R. C. (2000). Posttraumatic stress disorder: the burden to the individual and to society. Journal of Clinical Psychiatry, 61: 4-14
Ipser, J. C., & Stein, D. J. (2012). Evidence-based pharmacotherapy of post-traumatic stress disorder (PTSD). Int J Neuropsychopharmacol, 15: 825-840
Bradley, R., Greene, J., Russ, E., Dutra, L., & Westen, D. (2005). A multidimensional meta-analysis of psychotherapy for PTSD. Am J Psychiatry, 162: 214-227
DeGiorgio, C. M., Murray, D., Markovic, D., & Whitehurst, T. (2009). Trigeminal nerve stimulation for epilepsy: long-term feasibility and efficacy. Neurology, 72: 936-938
Schrader, L. M., Cook, I. A., Miller, P. R., Maremont, E. R., & DeGiorgio, C. M. (2011). Trigeminal nerve stimulation in major depressive disorder: first proof of concept in an open pilot trial. Epilepsy Behav, 22: 475-478
Jean, A. (1991). The nucleus tractus solitarius: neuroanatomic, neurochemical and functional aspects. Arch Int Physiol Biochim Biophys, 99: A3-A52
Cook, I. A., Schrader, L. M., Degiorgio, C. M., Miller, P. R., Maremont, E. R., & Leuchter, A. F. (2013). Trigeminal nerve stimulation in major depressive disorder: acute outcomes in an open pilot study. Epilepsy Behav, 28: 221- 226
Sui, L., Huang, S., Peng, B., Ren, J., Tian, F., & Wang, Y. (2014). Deep brain stimulation of the amygdala alleviates fear conditioning-induced alterations in synaptic plasticity in the cortical-amygdala pathway and fear memory. J neural Transmission, 121: 773-782
Shiozawa, P., da Silva, M. E., Netto, G. T., Taiar, I., & Cordeiro, Q. (2015). Effect of a 10-day trigeminal nerve stimulation (TNS) protocol for treating major depressive disorder: a phase II, sham-controlled, randomized clinical trial. Epilepsy Behav, 44: 23-26